
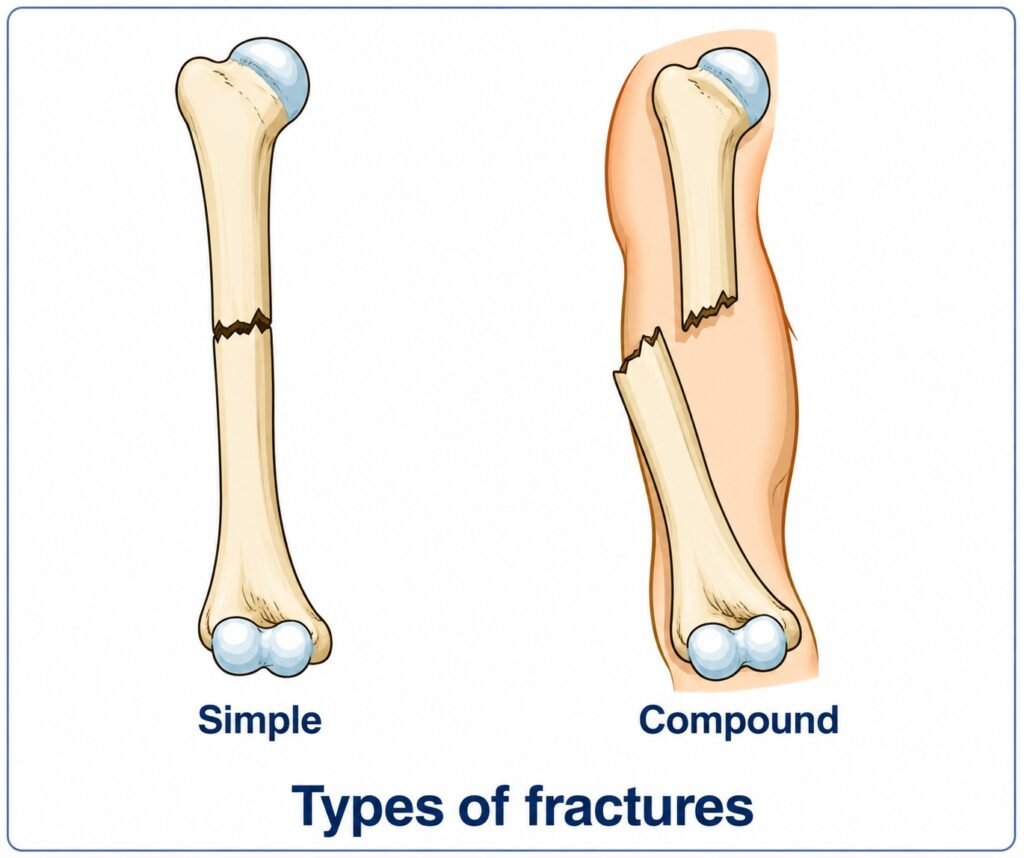
A fracture is a break in a bone. The bone may break into two or more pieces or may develop a linear crack. Fractures are classified as closed if the skin remains intact. If there is a wound at or near the fracture site, it is called an open fracture.
Improper handling of a patient can convert a simple fracture into a compound one by forcing sharp bone ends through the skin. Open fractures with significant bleeding may lead to shock, especially when large bones are involved.
Indications of a fracture include:
- A heavy blow or force applied to the body or limbs.
- The casualty or others may have heard the bone break.
- Severe pain, especially on pressure or movement at the site.
- Distortion: Compare the injured limb with the uninjured one to detect swelling, bending, twisting, or shortening.
- Irregularity: The uneven edges of a broken bone may be visible in an open fracture or felt under the skin in a closed fracture.
- Loss of use: The casualty may be unable or unwilling to use the injured part due to pain. Even slight movement may cause severe pain. Facial expressions may indicate discomfort. In some cases, when bone ends are impacted, limited use may still be possible but painful.
- Abnormal movement and grating of bone ends: These should not be deliberately tested. A limb may feel unstable, and a grating sensation may occur when support is attempted. Either sign confirms a fracture.
- Swelling: The affected area may be swollen and bruised due to internal bleeding. Swelling usually appears immediately, followed by skin discoloration.
General treatment
RADIO MEDICAL ADVICE should be sought early in cases of open fractures or severe fractures (such as skull, femur, pelvis, or spine), as evacuation from the ship may be necessary.
Unless there is immediate danger, the patient should not be moved until bleeding is controlled and fractures are immobilized with splints.
Bleeding
Bleeding from open fractures should be controlled by applying pressure and dressing the wound. Bleeding originates from surrounding tissues, not from the bone itself. Care must be taken when elevating a fractured limb, but elevation is recommended if bleeding is severe. Blood loss can be fatal, whereas a fracture alone is not. Rest is essential to prevent further bleeding, additional injury, and pain.
Once bleeding is controlled, the wound may be treated. Clean the surrounding area thoroughly with soap and water, then disinfect with a 1% (10 g/litre) cetrimide solution. Do not allow the cleaning solution to enter the wound. The wound itself should not be washed. Cover it with a sterile dressing.
Foreign particles such as dirt or debris should be gently removed using sterilized forceps. Blood clots should not be disturbed, as this may restart bleeding. The wound should not be stitched. Dressings should remain in place for 4–5 days if there is no infection.
Pain
If the patient is experiencing severe pain, 10 mg of morphine sulfate may be given by intramuscular injection. Before repeating the dose, RADIO MEDICAL ADVICE must be obtained. Avoid unnecessary movement or rough handling of the injured area.
Immobilization
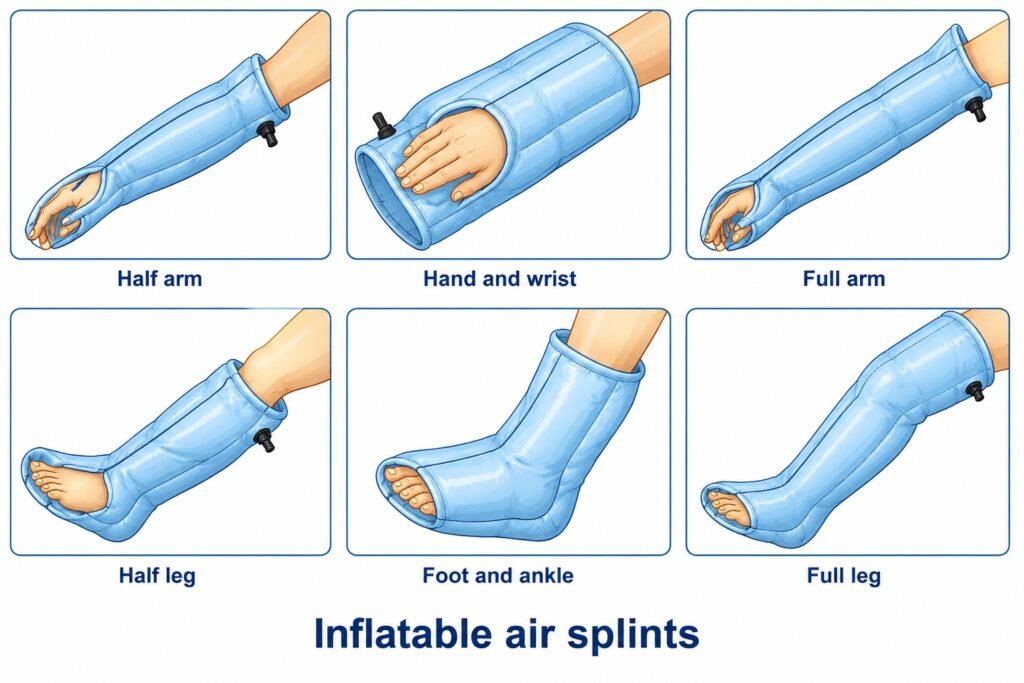
Inflatable splints can be used for temporary immobilization of limb fractures but are not suitable for fractures located far above the knee or elbow, as they do not provide sufficient support in these areas.
The splint is placed around the limb and inflated by mouth. Other inflation methods may overinflate the splint and restrict circulation. Inflatable splints can be applied over wound dressings.
These splints are made of transparent plastic, allowing observation of bleeding. Care must be taken to keep sharp objects away to prevent puncture.
To ensure proper stabilization, the splint must extend beyond the joints at both ends of the fractured bone.
Inflatable splints may be used during transport within the ship or to a hospital but should not remain in place for more than a few hours. After that, alternative methods of immobilization should be used.
Immobilize the limb in the position in which it is found, if comfortable. If movement is necessary due to poor circulation or other reasons, apply gentle and steady traction by pulling the limb away from the body before repositioning it.
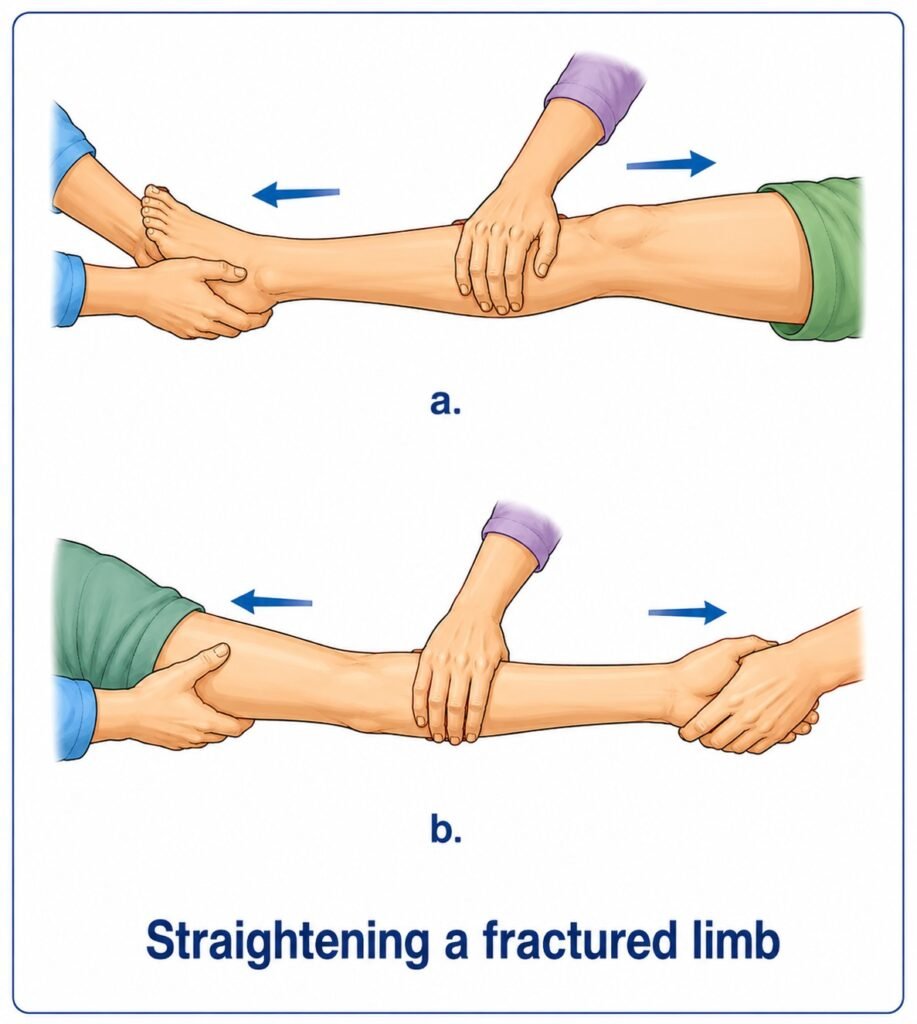
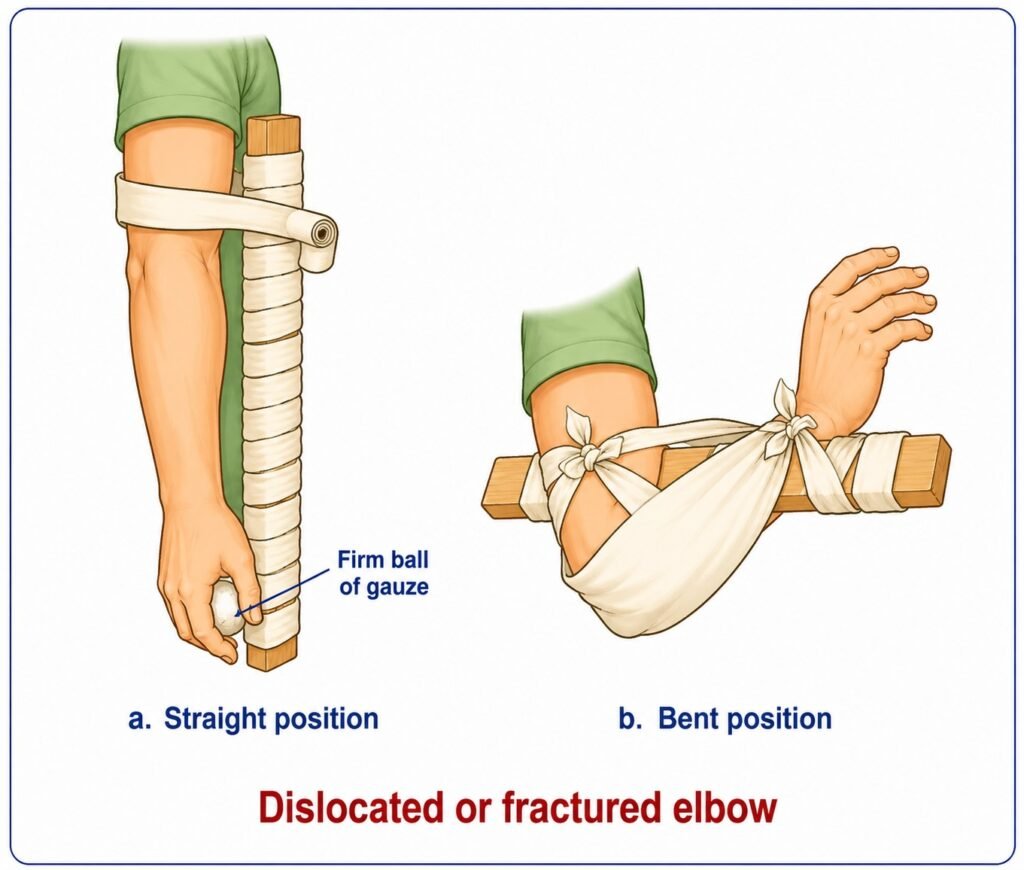
If a long bone in the arm or leg is fractured, it may be carefully straightened by applying traction at the hand or foot and realigning the limb. However, fractures involving joints, such as the elbow or knee, should not be manipulated. They should be positioned carefully for splinting. The knee should be splinted in a straight position, and the elbow at a right angle.
Circulation of the blood
Check and recheck blood circulation in a fractured limb by pressing on a fingernail or toenail. When circulation is normal, the nail turns white when pressed and returns to pink when released. Continue checking until you are satisfied that circulation is adequate.
Danger signs include:
- Bluish or pale (white) colour of the fingers or toes.
- Coldness in the area below the fracture.
- Loss of sensation below the injury (test by lightly touching the fingers or toes and asking the casualty if they can feel it).
- Absence of pulse.
If there is any doubt about circulation, immediately loosen all tight, limb-encircling dressings and gently straighten the limb, using traction while doing so. Then check circulation again. If the limb does not become warm and pink, and no pulse can be detected, urgent medical assistance is likely required to prevent amputation. Obtain RADIO MEDICAL ADVICE.
Remember that fractures may cause serious internal bleeding. Monitor carefully and take appropriate action.
Fractures of specific body areas
Skull
A skull fracture may result from a fall, a direct blow, a crushing injury, or a penetrating injury such as a bullet wound. The patient may be conscious, unconscious, or dizzy, and may experience headache or nausea. There may be bleeding from the nose, ears, or mouth, along with possible paralysis and signs of shock.
Treatment. Immediate care is essential to prevent further brain injury. Keep the patient lying down. If the face is flushed, slightly elevate the head and shoulders. If the face is pale, keep the head level with or slightly lower than the body. Bleeding may be controlled by applying direct pressure to the temporal or carotid arteries. Move the patient carefully, supporting the head on both sides with sandbags.
Morphine sulfate must never be given.
Upper jaw
In all facial injuries, maintaining a clear airway is the first priority.
Treatment. Control any bleeding from wounds. Loose teeth should not be removed without RADIO MEDICAL ADVICE unless there is a risk that they may be swallowed or obstruct the airway.
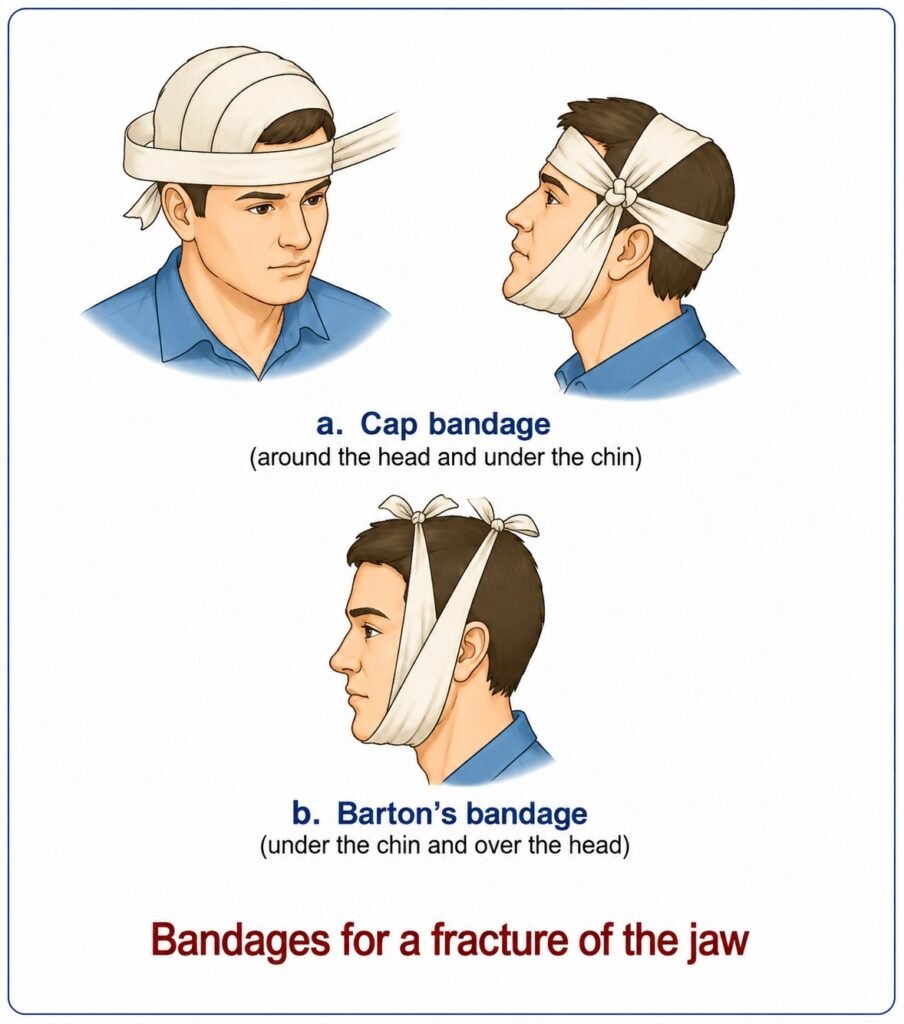
Lower jaw
A fracture of the lower jaw may cause deformity, missing or uneven teeth, bleeding from the gums, swelling, and difficulty swallowing.
Treatment. The injured jaw may obstruct breathing. If this occurs, pull the jaw and tongue forward and maintain this position.
If both sides of the jaw are fractured, the jaw and tongue may fall backward and block the airway. Place a finger (yours or the casualty’s) behind the lower front teeth and pull the jaw and tongue forward. If possible, position the casualty sitting upright with the head leaning forward. Clenching the teeth may help prevent further movement.
If the casualty cannot sit due to other injuries, place them in the unconscious position. Another person must stay with them, maintaining the forward position of the jaw if needed and closely observing breathing.
Jaw fractures usually cause limited movement because pain induces muscle spasm, keeping the teeth clenched and the jaw immobilized.
Apply cold compresses to reduce swelling and pain. Immobilize the jaw by keeping the mouth closed and applying a bandage.
If the casualty is unconscious, bleeding from the mouth, or at risk of vomiting, someone must remain present at all times to loosen the bandage if necessary.
Treat for pain.
Collar bone, shoulder blade, and shoulder
Fractures in these areas commonly result from a fall onto an outstretched hand or directly onto the shoulder. Direct impact is a less frequent cause.
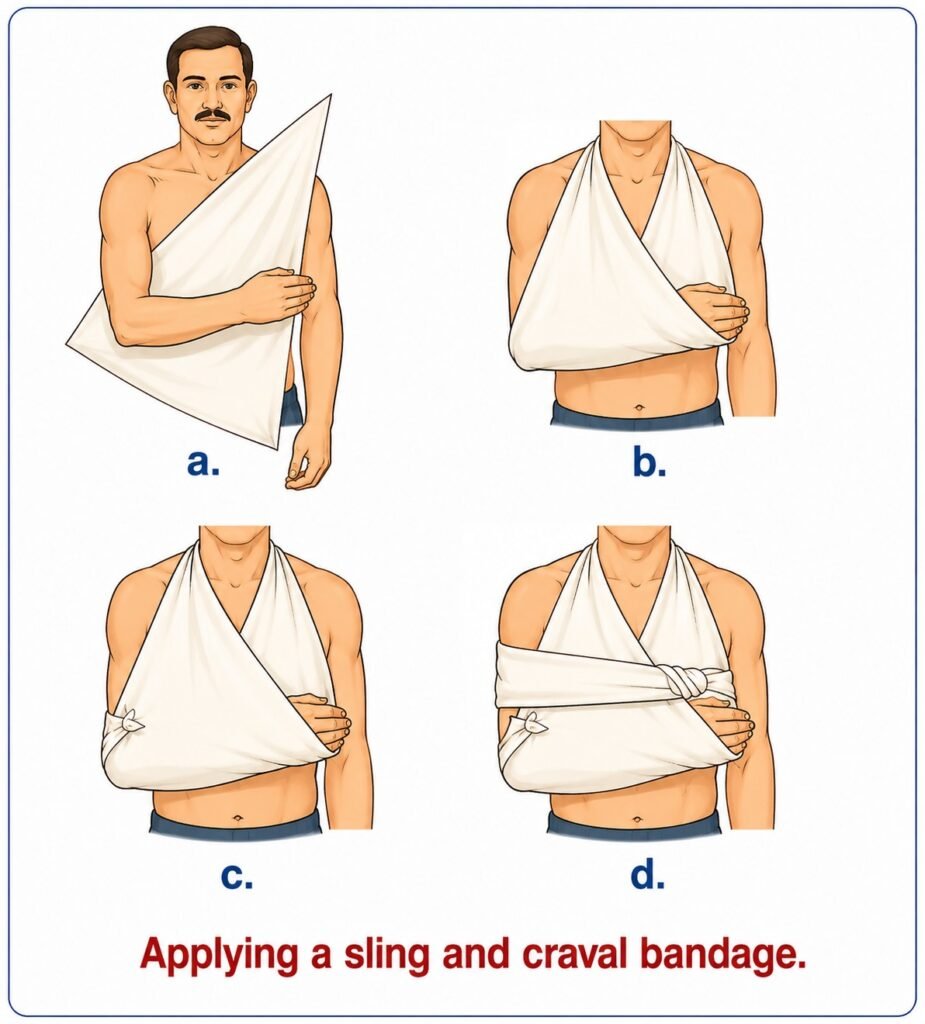
Place a pad about the size of a fist in the armpit. Then secure the arm to the body, for example using a triangular sling. Keep the casualty in a sitting position, as this is usually more comfortable.
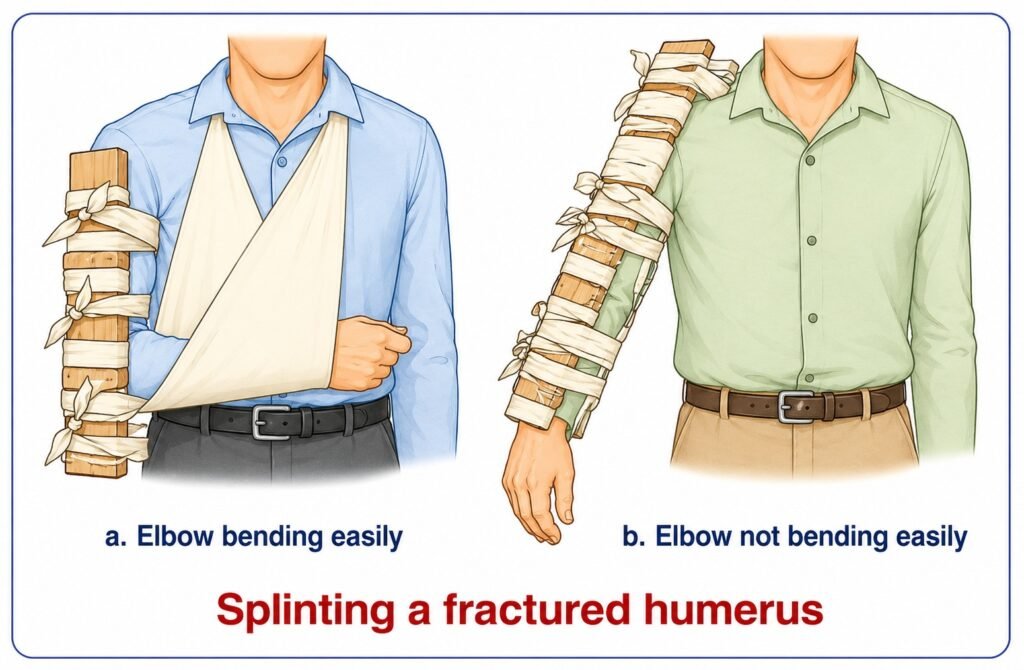
Upper arm (humerus) and the elbow
Fractures of the humerus may involve complications due to nearby nerves and blood vessels. Symptoms include pain, tenderness, deformity, and inability to lift the arm or bend the elbow.
Treatment. Apply a full-arm inflatable splint if available. If not, place the arm in a sling and secure it to the body with a wide bandage. A short padded splint may also be applied to the outer side of the arm.
Do not bend the elbow if it does not move easily. Apply long padded splints to both the inner and outer sides of the arm. If the elbow joint may be involved, immobilize it with a splint.
Treat for pain.
Lower arm (radius and ulna) or forearm
The forearm contains two bones, either or both of which may be fractured. If only one bone is broken, the other may act as a splint, resulting in minimal deformity. However, fractures near the wrist often show visible deformity. When both bones are broken, deformity is usually obvious.
Treatment. Carefully straighten the fracture by applying traction to the hand.
Apply a half-arm inflatable splint if available. If not, use two well-padded splints—one on top and one underneath the forearm—extending from above the elbow to the middle of the fingers.
Raise the hand about 10 cm higher than the elbow and support the arm in a sling.
Wrist and hand
A wrist fracture often results from a fall on an outstretched hand and typically presents with a lump-like deformity on the back of the wrist, along with pain, tenderness, and swelling.
Do not attempt to straighten or manipulate a wrist fracture. Treat it similarly to a forearm fracture.
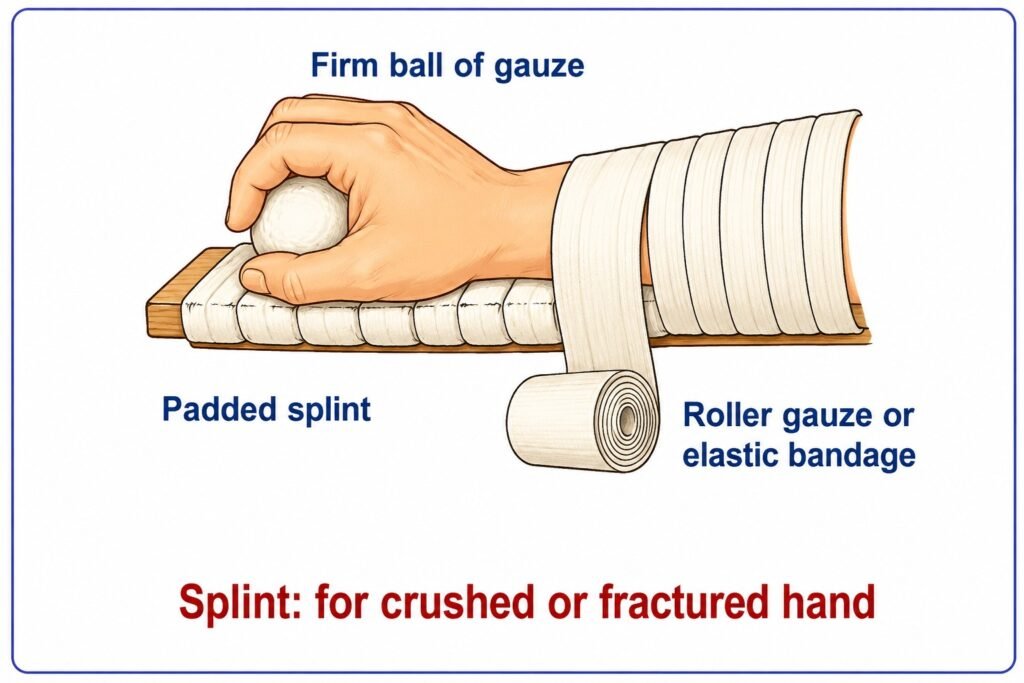
Hand injuries may result from direct blows or crushing forces. Symptoms include pain, swelling, reduced movement, open wounds, and fractures.
Place the hand on a padded splint extending from the mid-forearm to beyond the fingertips. Position a firm roll of gauze under the fingers to maintain a natural curved (cupped) position.
Secure the hand with bandage and support it in a sling. Further treatment is often urgently required to preserve hand function. Obtain RADIO MEDICAL ADVICE.
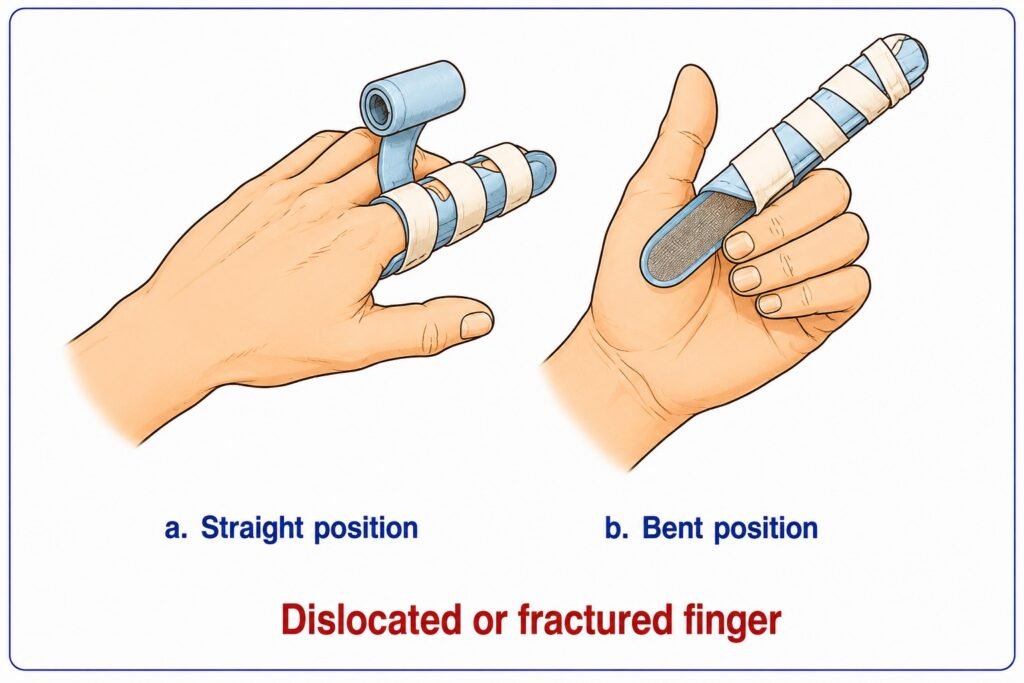
Finger
Only the injured finger should be immobilized, while allowing movement of the others.
Straighten the finger by holding the wrist with one hand and gently applying traction to the fingertip with the other. Immobilize the finger with a splint.
The patient should be examined by a physician as soon as possible.
Spine
A FRACTURED SPINE IS A VERY SERIOUS INJURY. IF A SPINAL FRACTURE IS SUSPECTED, INSTRUCT THE CASUALTY TO REMAIN STILL AND DO NOT ALLOW ANYONE TO MOVE THEM UNTIL THEY ARE SUPPORTED ON A HARD, FLAT SURFACE.
Improper handling of a spinal injury may damage the spinal cord, leading to permanent paralysis, loss of sensation in the legs, and lifelong loss of bladder and bowel control. Falls from height are a common cause of spinal injuries at sea. Always suspect a spinal fracture if a person has fallen more than two metres.
Ask about back pain. Most patients with spinal fractures feel pain, but some may not. Assess the mechanism of injury carefully and treat as a spinal fracture if in doubt. Ask the casualty to move their toes and check for sensation by touching them.
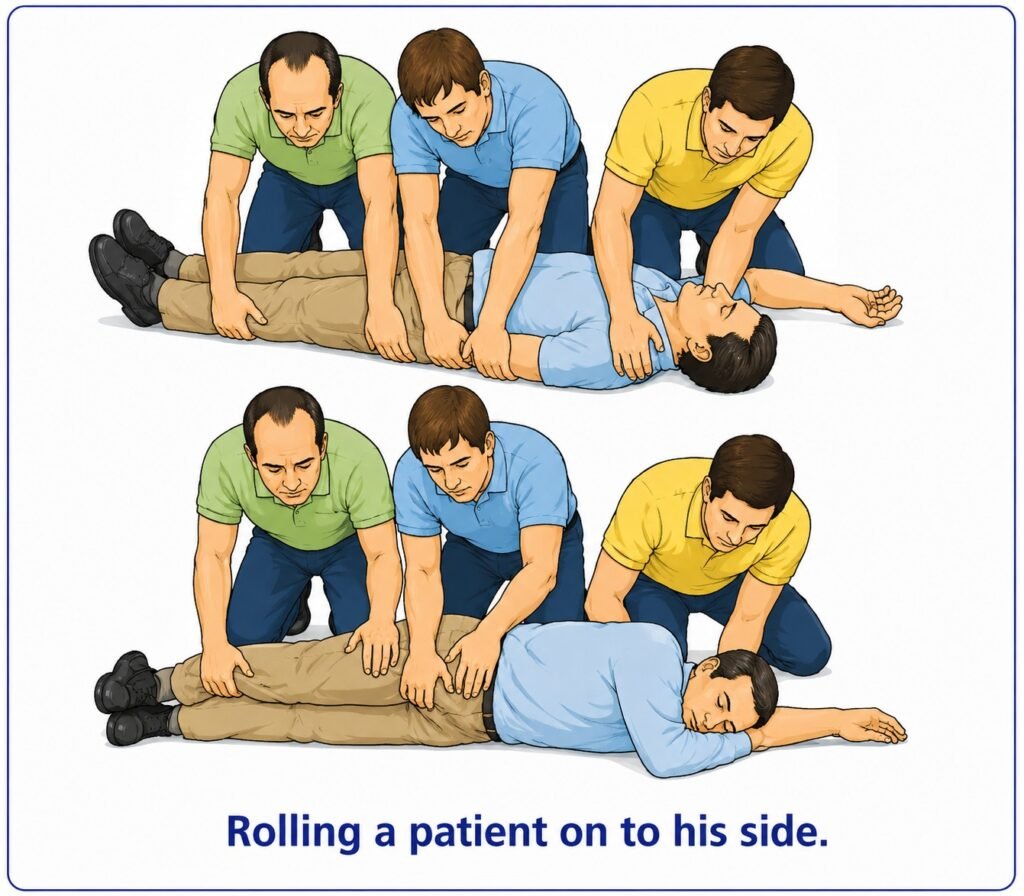
The casualty must be kept straight and still at all times. Never bend or lift them by the knees and shoulders. However, they may be carefully rolled onto their side if done gently, as this causes minimal spinal movement.
The goal of first aid is to place the casualty on a firm, flat surface with full spinal support and keep them in that position until X-rays can be performed.
Immediately instruct the casualty not to move. Improper movement may cause permanent paralysis.
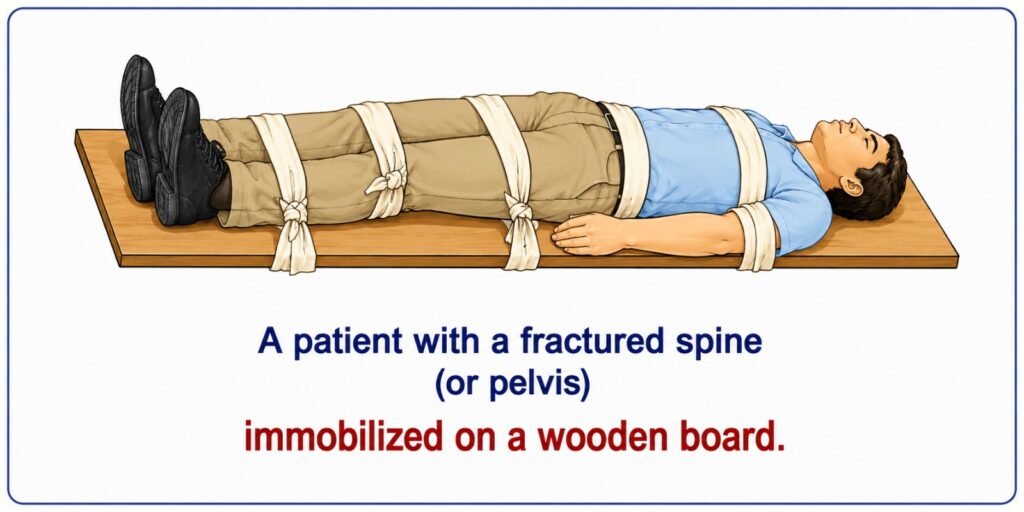
Secure the feet and ankles together using a figure-of-eight bandage. Use traction at the head and feet to gently straighten the body. Do not bend the casualty.
Prepare a rigid stretcher. A Neil-Robertson or basket stretcher is suitable. A canvas stretcher alone is not suitable unless reinforced with rigid boards. Some stretchers may require additional stiffening.
If no stretcher is available, a wide wooden board may be used. This method is also suitable for suspected pelvic fractures.
Another method involves rolling the casualty carefully onto a blanket, then tightly rolling the edges of the blanket alongside the body. Prepare a stretcher with rigid support and padding to fill the natural curves of the spine (one pad for the lower back and a smaller one for the neck).
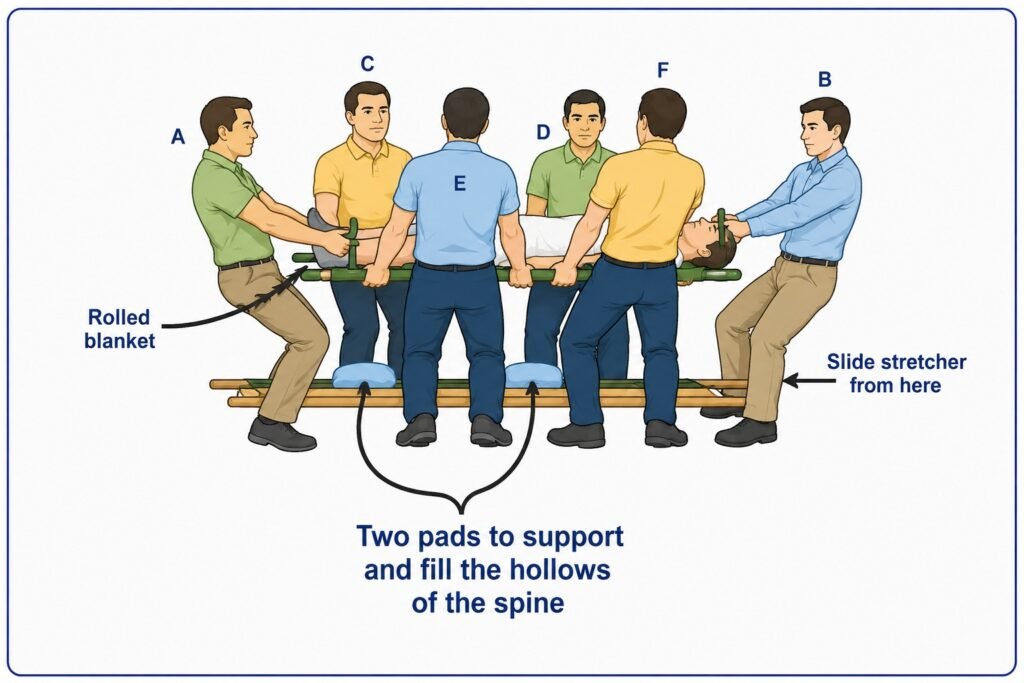
To lift the casualty:
- At least two people should hold each side of the blanket.
- One person should be at the head and one at the feet to apply traction.
- Additional help is needed to position the stretcher.
Apply steady traction to the head and feet. Lift the casualty slowly and carefully just high enough to slide the stretcher underneath. Keep the body straight at all times.
Position the stretcher correctly beneath the casualty and adjust the padding to support the spine.
Lower the casualty very slowly onto the stretcher, maintaining traction until fully supported.
The casualty can then be transported. If transferring to another surface, it must also be firm and flat, and the same precautions must be followed.
Because many people may be involved in handling the casualty, it may be helpful for one person to read instructions aloud during the process to ensure careful coordination.
Refer to Stroke and paralysis for further guidance on managing spinal cord injuries.
Neck
Injuries to the neck are often compression fractures of the vertebrae. These may occur, for example, when a person suddenly stands up and strikes their head forcefully, or when an object falls onto the head. Falls from a height can also cause neck injuries. Treatment is similar to that for spinal fractures, as the neck is the upper part of the spine.
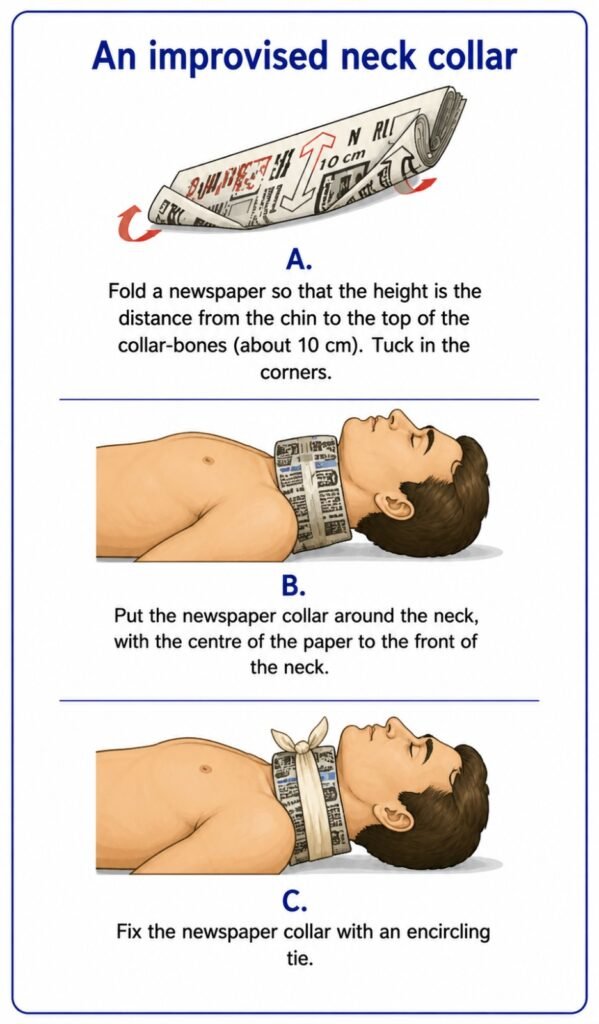
The casualty should be laid flat if not already in this position and must be kept still and straight. A neck collar should then be gently applied to prevent movement, while an assistant stabilizes the head.
An improvised neck collar can be made from a newspaper. Fold the newspaper so that it is about 10 cm wide at the front. Fold the top edge slightly to make the back narrower. Tie it around the neck so that the top edge rests under the chin and the bottom edge lies over the collarbones. Secure it in place with a bandage, scarf, or necktie. This will help keep the neck immobilized.
Chest
Rib injuries often result from falling against a sharp or angled object. Severe injuries may also result from strong blows to the chest or falls from a height.
Sharp pain from broken ribs may be felt, worsening with breathing movements. Lung damage may be indicated if the casualty coughs up bright red, frothy blood.
If there is an open chest wound (sucking wound), it must be sealed immediately. Otherwise, air will enter the chest cavity, preventing the lungs from inflating due to loss of internal pressure. Apply a large dressing over the wound and seal it with wide adhesive plaster to make it airtight.
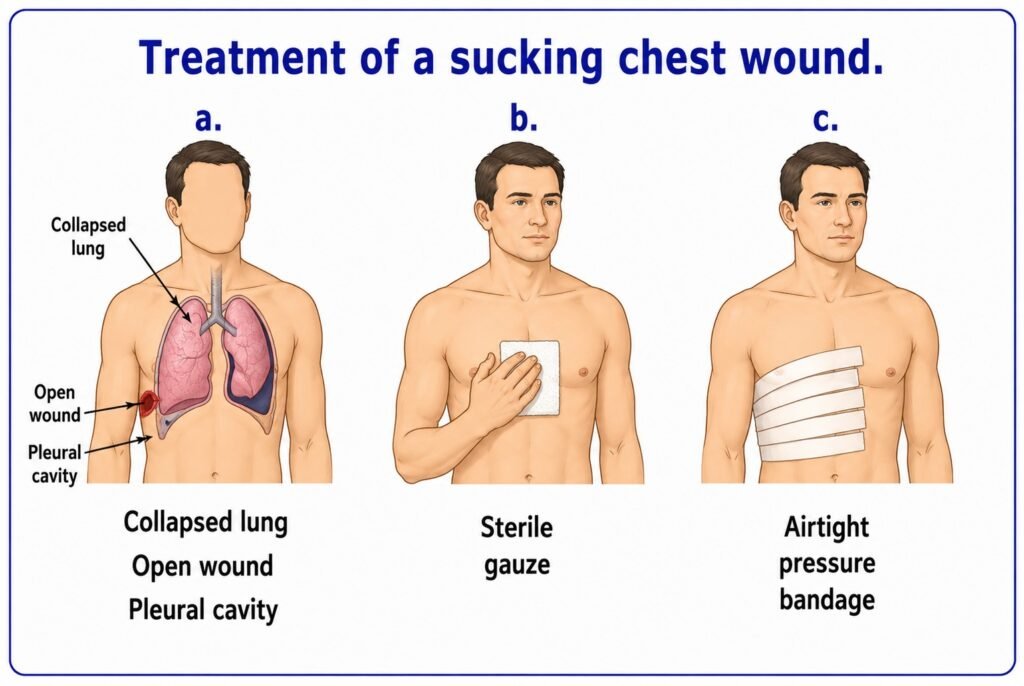
A suitable dressing can be made by applying petroleum jelly to gauze, covering it with aluminium foil or polythene, and placing it over the wound. Secure it tightly with adhesive plaster. A wet dressing may also be used. If nothing else is available, use the casualty’s bloodstained clothing temporarily to plug the wound.
Bleeding should be controlled by applying pressure at the source. In all chest injuries, begin a pulse chart early to monitor for internal bleeding. Record the respiratory rate as well.
Conscious casualties with chest injuries should be placed in a sitting position to aid breathing. If sitting is not possible, use a half-sitting position, supported with pillows or leaning forward. If possible, the casualty should lean toward the injured side to reduce movement, ease pain, and limit internal bleeding.
Unconscious casualties should be placed in the unconscious position, lying on the injured side. This reduces movement and helps limit internal bleeding. A slight head-down tilt may help keep the airway clear through drainage. If frothy blood is present in the mouth or nose, remove it using suction if available, or by wiping it away to keep the airway clear.
Pelvis
A pelvic fracture usually results from a fall from a height or direct force to the pelvic area. The casualty may complain of pain in the hip, groin, pelvis, lower back, or buttocks.
The ring compression test may be used: gently press inward and downward on both hip bones to compress the pelvis. Sharp pain or movement suggests a fracture.
If a pelvic fracture is suspected, instruct the casualty not to urinate. If urination occurs, collect the sample and check for blood. Damage to the bladder or urethra may allow urine to leak into surrounding tissues.
Pelvic fractures can cause severe internal bleeding. Begin a pulse chart immediately and monitor for hidden blood loss.
Handle the casualty with extreme care. If there is severe pain, use the same handling method as for spinal injuries before placing the casualty on a stretcher or board. Keep the casualty in the most comfortable position—on the back, side, or face down.
Treat for shock if necessary, but do not place the casualty in the shock position.
Use a rigid stretcher or wooden board for transport. Do not roll the casualty, as this may worsen internal injury. Place padding between the thighs and secure the knees and ankles together.
Hip to knee
A fractured thigh bone (femur) is a serious injury and may result in significant blood loss. Combined injuries may increase blood loss to life-threatening levels.
There is severe pain in the groin, and the casualty may be unable to lift the leg. The leg may appear shortened and rotated outward. Shock is common.
Obtain RADIO MEDICAL ADVICE.
A fracture of the neck of the femur causes shortening of the leg and outward rotation of the limb. Fractures of the shaft are usually easier to identify.
If a fracture is suspected, place padding between the thighs, knees, legs, and ankles. Carefully bring the uninjured leg toward the injured one. If this causes pain, apply gentle traction first. Bring the feet together and secure them with a figure-of-eight bandage.
Apply a padded splint from the armpit to beyond the foot and another from the groin to beyond the foot. Secure with ties and bind both legs together for support. Transport the casualty on a stretcher or board.
Knee
Knee fractures usually result from falls or direct blows. In addition to typical fracture signs, a groove may be felt in the kneecap. The casualty will be unable to extend the leg and may drag it while attempting to walk.
Treatment. Carefully straighten the leg. Apply a full-leg inflatable splint if available. Otherwise, use a padded board splint with support under the knee and ankle. Secure it with ties.
Lower leg (tibia and fibula)
Fractures of the lower leg are common. When both bones are broken, deformity is obvious. If only one bone is broken, the other may act as a splint, reducing visible deformity. Fractures of the tibia often result in open wounds. Swelling is common, and pain may require morphine sulfate.
Treatment. Gently straighten the leg using traction. Apply a full-leg inflatable splint if available. Otherwise, use padded splints on both sides and underneath the leg, extending from mid-thigh to beyond the heel.
Both legs
Fractures of both legs may involve severe blood loss. Monitor for shock and treat accordingly.
Prepare padded splints extending from thigh to ankles (or from armpit to ankles for higher fractures). Pad between the legs and bring the feet together gently, using traction if necessary. Secure with a figure-of-eight bandage.
Apply splints to the outer sides of both legs and secure with bandages. Avoid tying over fracture sites. Check circulation and sensation in the toes. Transport the casualty flat and straight on a stretcher.
Treat for pain.
Ankle and foot
Fractures of the ankle or foot are usually caused by falls, twisting injuries, or direct blows. Pain, swelling, and loss of function are common.
Treatment. Apply a half-leg inflatable splint if available. Otherwise, pad the ankle well and apply splints to both sides of the leg, extending from mid-calf to beyond the foot.