
Basic life support is an emergency life-saving procedure that involves recognizing and correcting failure of the respiratory or cardiovascular systems.
Oxygen, present in the atmosphere at about 21%, is essential for the life of all cells. The brain, the primary organ responsible for consciousness, begins to die if deprived of oxygen for as little as four minutes. The delivery of oxygen from the atmosphere to the brain cells requires two essential actions: breathing (intake of oxygen through the air passages) and circulation of oxygen-rich blood. Any serious disturbance in the airway, breathing, or circulation can quickly lead to brain death.
Basic life support consists of the “ABC” steps, referring to airway, breathing, and circulation.
Its prompt application is required in cases of:
A. Airway obstruction
B. Breathing (respiratory) arrest
C. Circulatory or cardiac (heart) arrest
Basic life support requires no instruments or supplies. Correct application of these steps can sustain life until the patient recovers sufficiently to be transported to a hospital, where advanced life support can be provided. Advanced life support includes specialized equipment, cardiac monitoring, defibrillation, maintenance of an intravenous line, and administration of appropriate drugs.
Basic life support must be carried out with the utmost urgency. Ideally, only seconds should pass between recognizing the need and beginning treatment. Any absence or inadequacy of breathing or circulation must be identified immediately.
If only breathing is inadequate or absent, it is sufficient to open the AIRWAY or provide ARTIFICIAL RESPIRATION.
If circulation is also absent, artificial circulation must be established through HEART COMPRESSION, combined with artificial respiration. If breathing stops before the heart stops, enough oxygen remains in the lungs to sustain life for several minutes. However, if the heart stops first, oxygen delivery to the brain ceases immediately. Brain damage may occur if the brain is deprived of oxygen for 4–6 minutes, and is highly likely beyond 6 minutes. This highlights the importance of rapid assessment and action.
Once basic life support has been started, it should not be interrupted for more than 5 seconds for any reason, except when it is necessary to move the patient; even then, interruptions should not exceed 15 seconds at a time.
Airway (Step A)
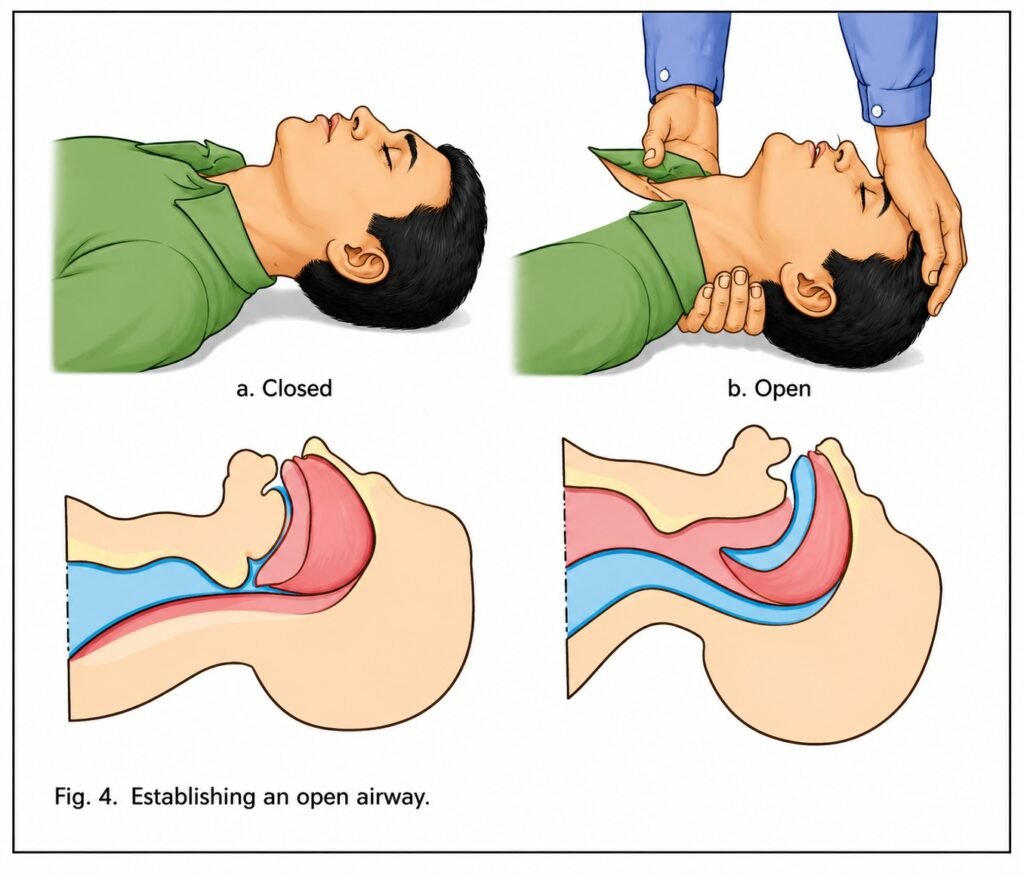
ESTABLISHING AN OPEN AIRWAY IS THE MOST IMPORTANT STEP IN ARTIFICIAL RESPIRATION. Spontaneous breathing may begin as a result of this simple action.
Place the patient face up on a firm surface. Position one hand under the patient’s neck and the other on the forehead. Lift the neck with one hand and apply pressure to the forehead with the other to tilt the head backward. This extends the neck and moves the base of the tongue away from the back of the throat. Maintain this position throughout artificial respiration and heart compression.
If the airway remains obstructed, remove any foreign material from the mouth or throat immediately using your fingers.
Once the airway is opened, the patient may or may not begin breathing again. To check for breathing, place your ear about 2–3 cm above the patient’s nose and mouth. If you can feel and hear airflow and observe chest and abdominal movement, breathing has resumed. Feeling and hearing are more reliable than seeing. In cases of airway obstruction, there may be no airflow even though the chest and abdomen move. Additionally, observing movement can be difficult if the patient is fully clothed.
Breathing (Step B)
If the patient does not quickly resume adequate spontaneous breathing after the
head has been tilted backward, artificial respiration should be provided using the mouth-to-mouth or mouth-to-nose method, or other techniques. Regardless of the method used, maintaining an open airway is essential.
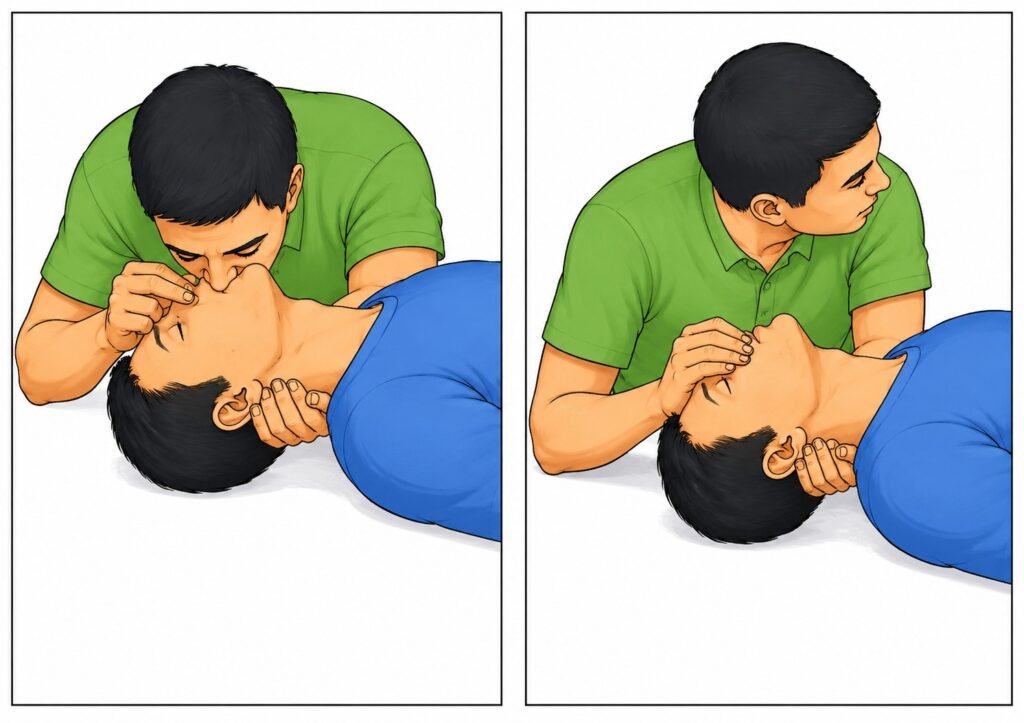
Mouth-to-mouth respiration
Keep the patient’s head tilted as far back as possible, with one hand placed under the neck.
Place the heel of the other hand on the forehead, with the thumb and index finger positioned toward the nose. Pinch the patient’s nostrils together using the thumb and index finger to prevent air from escaping.
Continue to apply pressure on the forehead with the palm to maintain the backward tilt of the head.
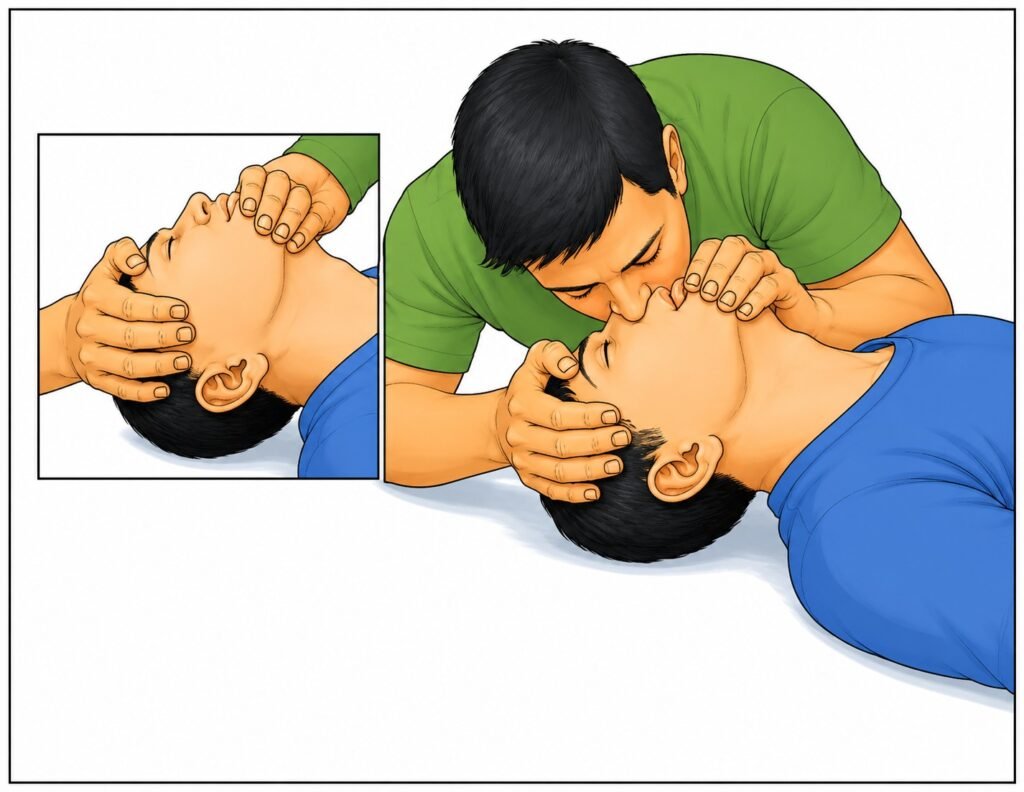
Take a deep breath, then form a tight seal with your mouth over and around the patient’s mouth.
Blow four quick, full breaths initially without allowing the lungs to fully deflate between breaths.
Watch the patient’s chest while inflating the lungs. If adequate respiration is occurring, the chest should rise and fall.
Remove your mouth and allow the patient to exhale passively. If you are correctly positioned, the patient’s exhaled air will be felt on your cheek. Take another deep breath, form a tight seal again around the patient’s mouth, and blow into the mouth. Repeat this procedure 10–12 times per minute (once every five seconds) for adults and children over four years of age.
If there is no air exchange and an airway obstruction is present, insert your fingers into the patient’s mouth and throat to remove any foreign material, then resume artificial respiration. A foreign body should be suspected if you are unable to inflate the lungs despite proper positioning and a tight air seal around the mouth or nose.
Mouth-to-nose respiration
The mouth-to-nose technique should be used when it is not possible to open the patient’s mouth, when the mouth is severely injured, or when a tight seal around the lips cannot be achieved.
Keep the patient’s head tilted backward with one hand. Use the other hand to lift the lower jaw in order to seal the lips.
Take a deep breath, seal your lips around the patient’s nose, and blow in forcefully and smoothly until the patient’s chest rises. Repeat this quickly four times.
Remove your mouth and allow the patient to exhale passively.
Repeat the cycle 10–12 times per minute.
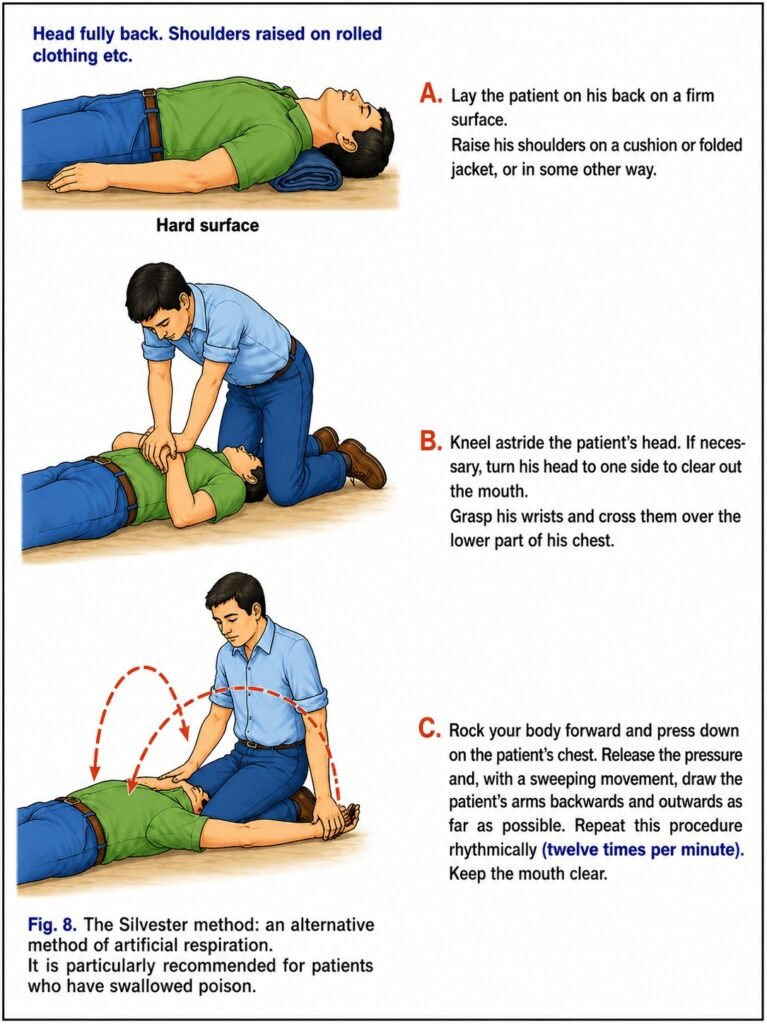
Alternative method of artificial respiration (Silvester method)
In some situations, mouth-to-mouth respiration cannot be used. For example, certain toxic or caustic substances may pose a risk to the rescuer, or facial injuries may prevent the use of mouth-to-mouth or mouth-to-nose techniques. In such cases, an alternative method of artificial respiration should be used. However, this method is much less effective than those described above and should only be used when mouth-to-mouth respiration cannot be performed.
Artificial respiration should be continued as long as there are signs of life; it may be necessary to continue for up to two hours or longer.
Heart compression (Step C)
When attempting to revive a non-breathing person whose heart has stopped beating, heart compression (external cardiac compression) must be performed together with artificial respiration.
Artificial respiration supplies oxygen to the lungs. From there, oxygen is carried by the circulating blood to the brain and other organs. Effective heart compression can temporarily restore blood circulation until the heart begins to beat again.
Technique for heart compression
Compression of the sternum produces some artificial ventilation, but not enough to adequately oxygenate the blood. Therefore, artificial respiration must always be provided when performing heart compression.
Effective heart compression requires enough pressure to depress the lower part of the sternum by about 4–5 cm in an adult. For chest compression to be effective, the patient must be placed on a firm surface. If the patient is on a bed, a board or other firm support should be placed under the back. However, chest compression should not be delayed while searching for such support.
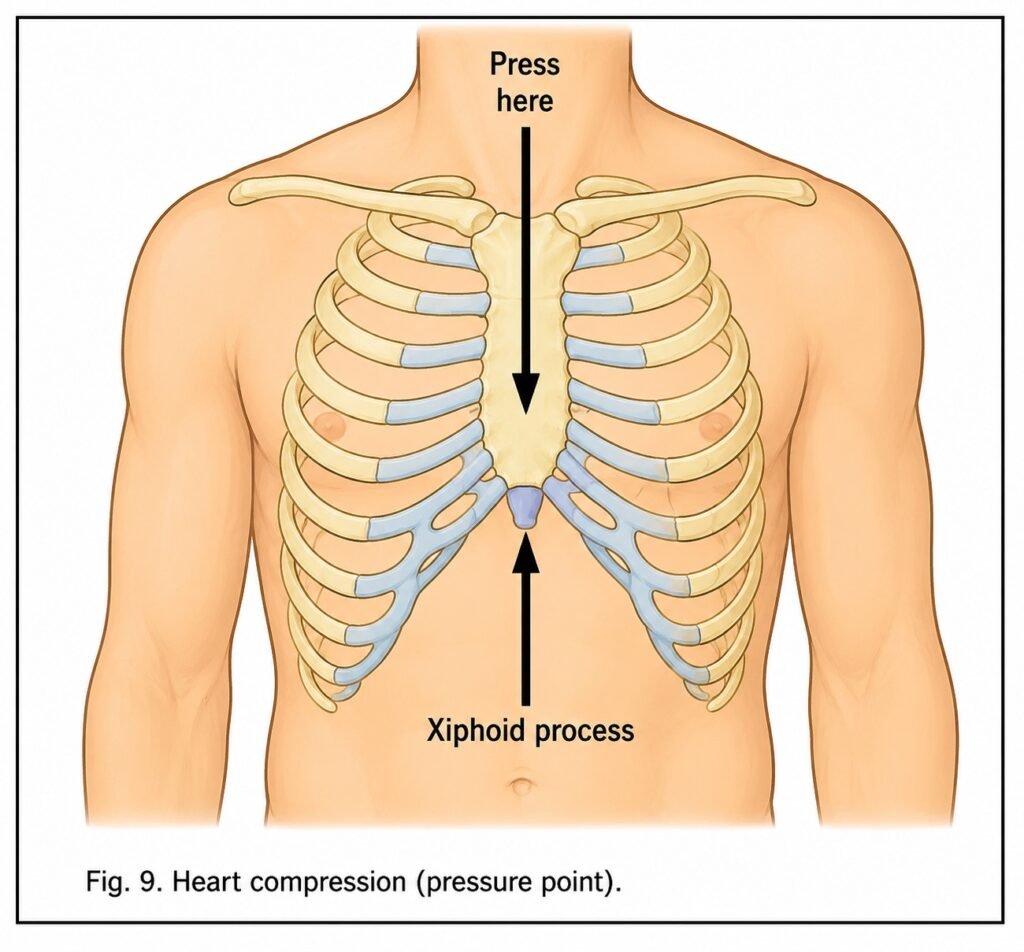
Kneel beside the patient and place the heel of one hand on the lower half of the sternum. Avoid placing the hand on the tip (xiphoid process) of the breastbone, which extends over the upper abdomen. Pressure on the xiphoid process may tear the liver and cause severe internal bleeding.
Locate the tip of the sternum and position the heel of your hand approximately 4 cm above it, toward the patient’s head. Your fingers must not rest on the patient’s ribs during compression, as this increases the risk of rib fractures.
Place the heel of the other hand on top of the first.
Lean forward so that your shoulders are almost directly above the patient’s chest.
Keep your arms straight and apply firm downward pressure to depress the lower sternum by 4–5 cm in an adult.
Compress the sternum at a rate of 60 times per minute for an adult (when another person is providing artificial respiration). This rate is sufficient to maintain blood flow while allowing the heart to refill between compressions. Compressions should be regular, smooth, and uninterrupted, with equal time for compression and relaxation. Under no circumstances should compression be interrupted for more than five seconds.
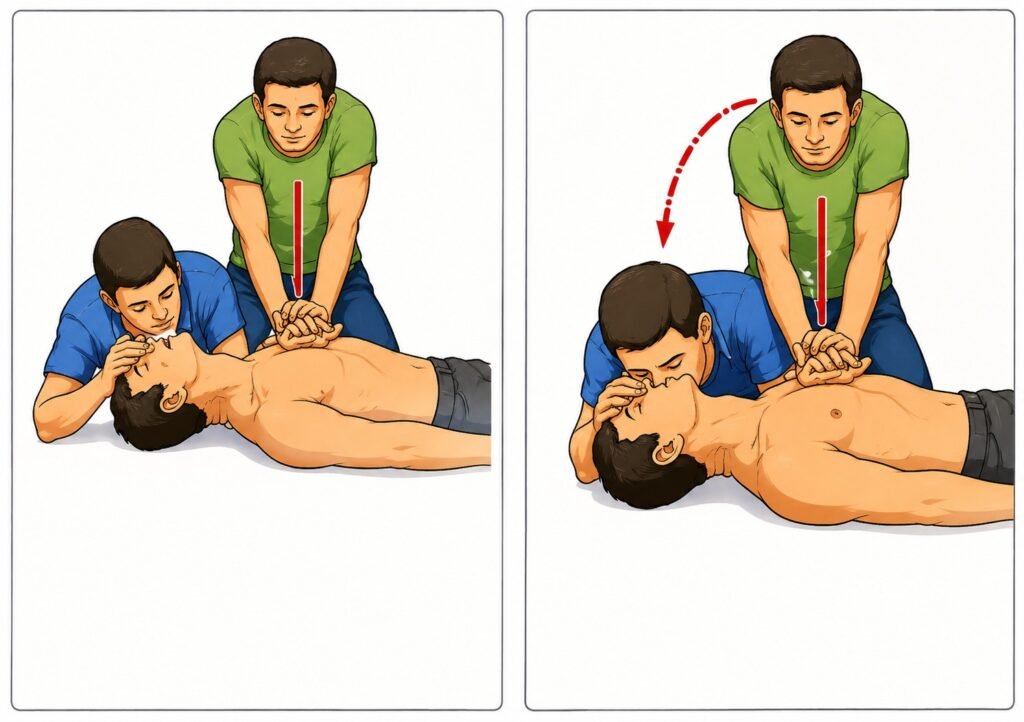
It is preferable to have two rescuers, as artificial circulation must be combined with artificial respiration. The most effective method is to give one breath after every five chest compressions (5:1 ratio). The compression rate should be 60 per minute when two rescuers are working together. One rescuer performs chest compressions, while the other remains at the patient’s head, maintains the head tilt, and continues artificial respiration. Breaths should be given without interrupting chest compressions, as any pause causes blood flow and pressure to drop to zero.
A single rescuer must perform both artificial respiration and chest compressions using a 15:2 ratio. Two quick breaths should be given after every 15 chest compressions, without waiting for full exhalation. A single rescuer must maintain a rate equivalent to 80 chest compressions per minute to achieve 50–60 effective compressions per minute, accounting for interruptions during breathing.
Checking effectiveness of heart compression: pupils and pulse
Check the pupils’ reaction. If the pupils constrict when exposed to light, this indicates that the brain is receiving adequate oxygen and blood. If the pupils remain widely dilated and do not respond to light, severe brain damage is likely to occur soon or may have already occurred. Dilated but responsive pupils indicate a less serious condition.
The carotid (neck) pulse should be checked after the first minute of heart compression and artificial respiration, and then every five minutes. The presence of a pulse indicates the effectiveness of chest compressions or the return of a natural heartbeat.
Other signs of effective resuscitation include:
- Expansion of the chest each time air is blown into the lungs.
- A pulse felt with each chest compression.
- Improvement in skin colour.
- Spontaneous gasping for breath.
- Return of a natural heartbeat.
Terminating heart compression
Deep unconsciousness, absence of spontaneous breathing, and fixed, dilated pupils for 15–30 minutes indicate brain death, and further attempts to restore circulation and breathing are usually unsuccessful.
In the absence of a physician, artificial respiration and heart compression should be continued until:
- The patient’s heart starts beating again and breathing is restored;
- Or the patient is transferred to a doctor or other qualified emergency medical personnel;
- Or the rescuer is unable to continue due to exhaustion.