
Burns and scalds
Burns and scalds are treated in the same manner, regardless of whether they are caused by dry heat or hot liquids. The skin consists of two layers: the outer epidermis and the deeper dermis, which contains glands, hair follicles, and nerve endings.
First-degree burns affect only the outer layer and cause redness, mild swelling, tenderness, and pain. Second-degree burns extend into the deeper layer and may cause severe redness, blisters, swelling, and fluid leakage. In deeper cases, distinguishing them from third-degree burns may be difficult initially. Third-degree burns involve the full thickness of the skin and may extend to deeper tissues. The skin may appear charred, white, or leathery, and pain may be absent due to nerve damage.
Burns can lead to significant fluid loss, mainly from the plasma component of blood. The severity of fluid loss depends more on the surface area affected than the depth. Greater fluid loss increases the risk of shock and places strain on the heart due to thicker blood.
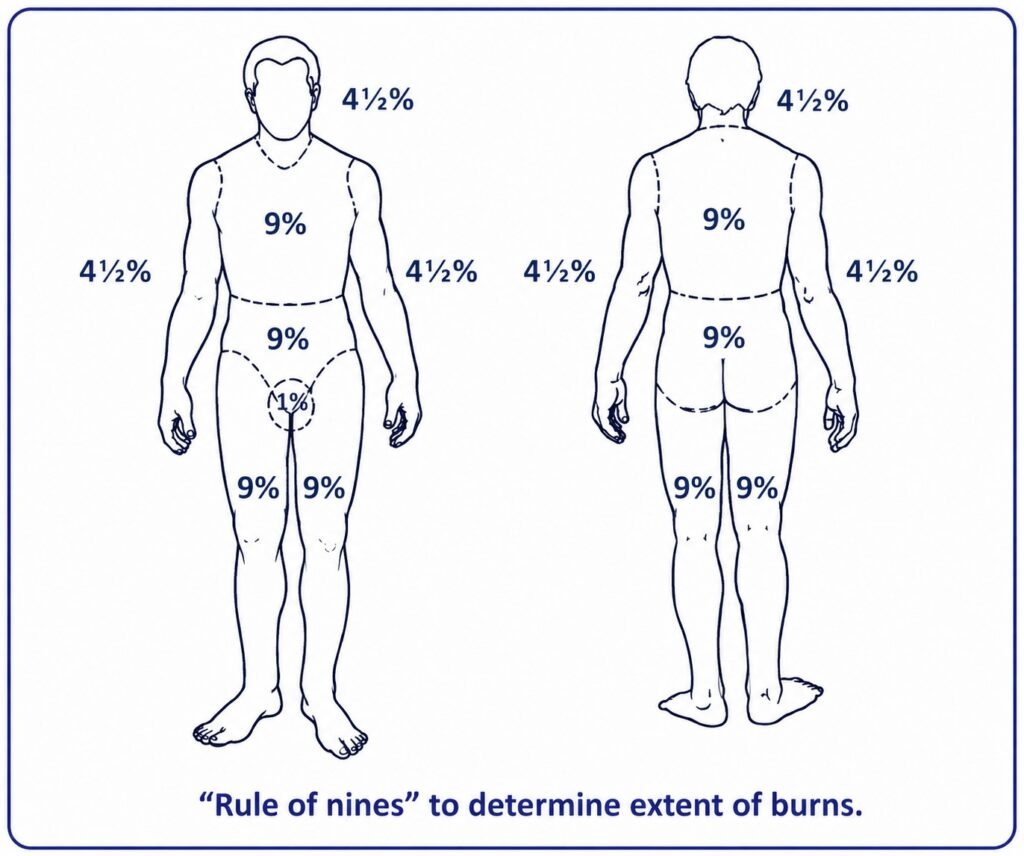
The extent of burns is commonly estimated using the “rule of nines,” which divides the body into sections representing percentages of total body surface area.
Severe burns require hospital treatment as soon as possible, especially in cases involving third-degree burns, infants, burns on the face or genital area, burns around joints, or large surface areas. While awaiting transfer, the patient should be kept in bed and encouraged to drink fluids, preferably oral rehydration solutions. If vomiting persists, intravenous fluids may be required. Pain relief and antibiotics should be administered, and anxiety may be managed with appropriate medication.
For less severe burns, treatment can be managed onboard. The affected area should be cleaned gently using soap and warm boiled water. Blisters should not be broken unless already ruptured, in which case dead skin should be carefully removed. The burn should then be covered with suitable ointment or sterile dressing, followed by absorbent layers and proper bandaging. Care should be taken to maintain cleanliness and prevent infection.
Dressings should generally remain in place for about a week unless signs of infection appear. First-degree burns usually heal within 7–10 days without scarring, while second-degree burns may take about three weeks to heal with minimal scarring.
Special burns
Severe sunburn with blistering should be managed in the same way as a first-degree burn, taking into account the extent of the body surface involved. In milder cases, the patient should be kept out of direct sunlight, and soothing applications such as calamine lotion or zinc ointment may be applied to relieve pain and irritation.
Burns or scalds affecting the mouth and throat require immediate rinsing with water, and the patient may be given ice to suck in order to reduce pain and swelling.
Respiratory burns occur when hot gases, smoke, or heated air particles are inhaled. Burns around the mouth, nose, face, neck, or singed hair may indicate involvement of the respiratory tract. Even in the absence of visible burns, heat from a flash fire can cause swelling in the upper airway. Mild cases may present with cough, hoarseness, or sore throat, whereas more severe cases may involve shortness of breath, persistent coughing, wheezing, and significant airway obstruction. In extreme cases, swelling may block the airway and lead to partial lung collapse. If breathing is difficult, an airway should be inserted immediately, and urgent medical advice must be obtained.