
Examination
All head injuries, except the most superficial ones, must be considered potentially dangerous, and therefore a careful examination is essential. Even small wounds should be examined thoroughly to ensure they are not associated with a skull fracture. The ears, nose, and throat must also be checked for the presence of blood or cerebrospinal fluid (CSF), which normally surrounds and cushions the brain and spinal cord. A casualty should be assumed to have sustained a serious head injury if there is any period of unconsciousness beyond a very short duration, if blood or fluid is seen leaking from the ears, nose, or throat, if there is suspicion of an open skull fracture, or if signs of brain damage such as paralysis are present. Additional warning signs include vomiting, increasing headache, confusion, drowsiness, abnormal behaviour, repeated loss of consciousness, or a slow pulse rate below 65 per minute.
Types of Head Injury
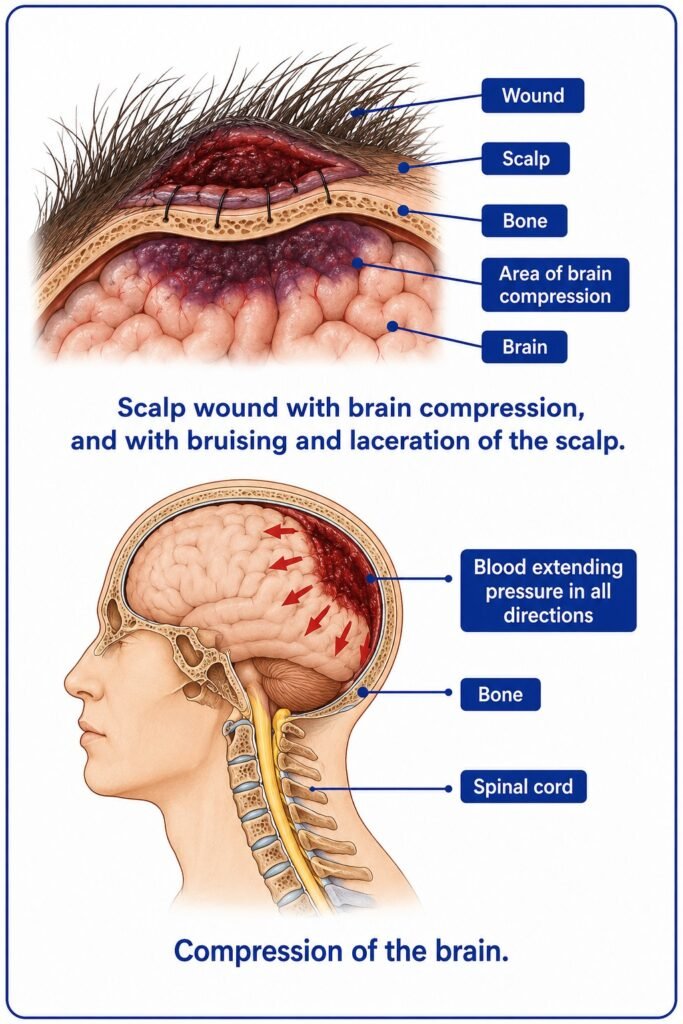
When a moderate force is applied to the head, bruising may occur. Because the scalp has a rich blood supply, a swelling or haematoma can form beneath it, which may feel firm and well-defined or soft and diffuse. Most blows to the head also result in wounds because there is little tissue between the scalp and the skull; these wounds tend to bleed heavily and may have ragged edges.
Concussion occurs when the brain is subjected to a heavy blow, causing temporary disturbance of its function. It is usually suspected when there is brief loss of consciousness, along with memory loss, headache, nausea, or vomiting. Skull fractures are classified into three types. Linear fractures affect the top and sides of the skull and are usually diagnosed only through X-ray. Fractures of the base of the skull occur due to indirect force and are often identified by leakage of blood or CSF from the ears, nose, or throat. Depressed fractures result from a heavy blow that drives fragments of bone inward, causing damage to brain tissue and internal bleeding; these may be felt during examination and may also involve open wounds.
Compression of the brain occurs when bleeding within the skull increases pressure and disrupts brain function. This condition may follow what initially appears to be a minor injury. Typically, there is a blow to the head, a brief loss of consciousness, apparent recovery, and then a gradual deterioration into coma. Symptoms may include twitching or seizures, noisy breathing, a slow pulse, unequal or dilated pupils, paralysis on one side of the body, and dangerously high body temperature.
Treatment
For bruising or haematoma, no specific treatment is usually required, although applying an ice pack may help control bleeding. Superficial wounds without fracture should be treated by applying pressure to stop bleeding and, if necessary, stitching the wound.
In cases of concussion, the casualty should be kept at rest in bed for at least 48 hours. Headaches may occur and can be treated with acetylsalicylic acid or paracetamol. The patient must be warned to report immediately if symptoms worsen, such as increasing headache, drowsiness, or vomiting, and should be examined by a doctor at the next port.
Serious head injuries, including fractures and brain compression, require urgent medical attention. If the ship is in port, the casualty should be transferred to a hospital immediately. If at sea, radio medical advice should be sought. Meanwhile, if the casualty is unconscious, he should be placed in the unconscious position and kept under constant observation to prevent complications such as vomiting or seizures. If a depressed fracture is suspected, bleeding should be controlled using a ring-pad.
In cases of open skull fractures, the wound must not be probed, pressed, or have bone fragments removed. Infection must be prevented by carefully cleaning the surrounding area, cutting hair around the wound, and applying sterile dressings such as petrolatum gauze, followed by padding and bandaging. Antibiotic treatment should be started, and if an allergic reaction occurs, appropriate medication should be given. Morphine must not be administered unless the head injury is minor and there are other severe injuries causing pain.